
How could nursing homes have done better?

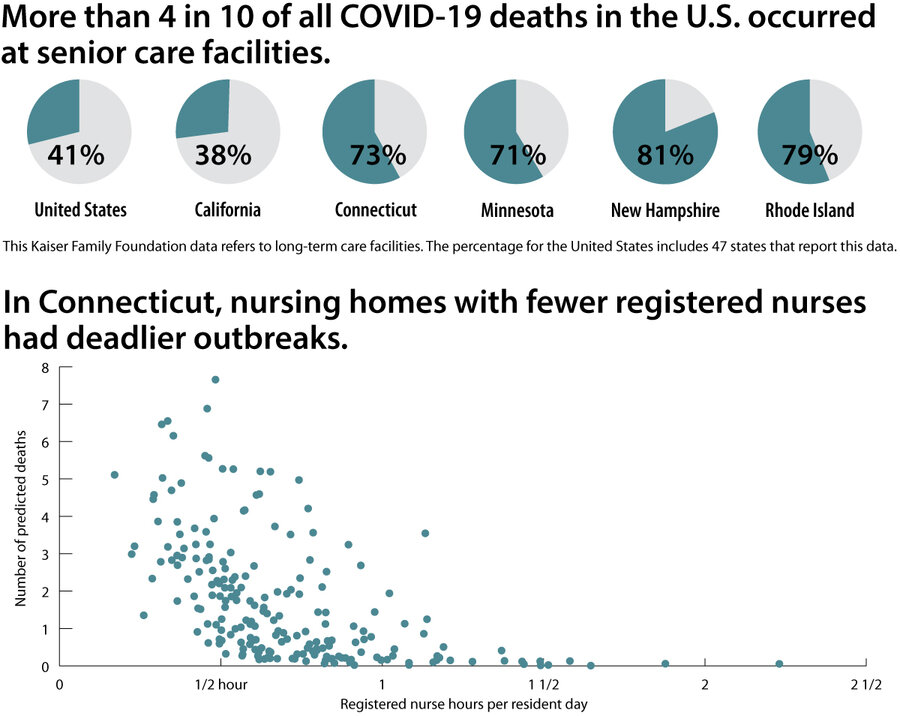
Nursing home residents have accounted for some 40% of all COVID-19 deaths in the United States. To some experts, this tragic toll was simply the result of location: in hotspots such as New York City. Even well-run, highly rated, long-term care facilities were hit hard. But other analyses point to a particular problem area: understaffed homes run for profit did worse at keeping their residents safe from the coronavirus. Two peer-reviewed studies of nursing homes in Connecticut and California separately found that low nurse-to-patient ratios, particularly of registered nurses, were associated with larger and deadlier COVID-19 outbreaks.
For instance, at RegalCare at Southport, a for-profit 120-bed facility in Connecticut, payroll data indicates that registered nurses provide less than half the state average of resident coverage. It’s been on a federal watch list for two years for a list of deficiencies, including poor infection control.
Why We Wrote This
Nursing home residents constitute a disproportionately large percentage of pandemic deaths. Here we take a look inside to see what might be improved.
By late July, RegalCare had lost 19 residents. A number of staff members caught the virus themselves.
Melinda Haschak was one of them. A licensed practical nurse, she testified before a House Ways and Means Committee hearing last month about RegalCare’s lack of staffing, shortage of personal protective equipment such as masks, and her perception that management didn’t support front-line employees.
Nurses are grateful for food donations, she said. But “my co-workers and I don’t need a pizza party. We need PPE,” she told the committee.
As Melinda Haschak responded to the Code Blue that blared through the intercom, she was missing a crucial piece of information.
The resident she was rushing to save had tested positive for the coronavirus.
Ms. Haschak knew that some of the residents in the Connecticut nursing home where she works as a licensed nurse had tested positive. But the fellow nurse who could have helped her most – who had begun to piece together the larger picture, who knew the resident in distress had tested positive, and whose concerns had been dismissed by management – was at home, recovering from the coronavirus herself.
Why We Wrote This
Nursing home residents constitute a disproportionately large percentage of pandemic deaths. Here we take a look inside to see what might be improved.
Before falling ill, Kennethe Polissaint had noticed that the first resident who tested positive and died in the hospital had never left the facility – meaning the nursing home staff itself was unwittingly spreading the virus and should be tested. Yet when she told the assistant director of nursing, a registered nurse, “they didn’t do anything about it,” Ms. Polissaint says.
Ms. Haschak was not able to save the Code Blue resident, who never regained consciousness.
And afterward, the senior nurses who oversee infection control didn’t send her home to isolate. Instead, she went back to her wing, which was supposed to be COVID-19-free.
Two weeks later, Ms. Haschak fell ill with COVID-19.
The pattern that played out in RegalCare at Southport has been mirrored at thousands of nursing facilities across the United States. More than 41% of the 186,000 Americans who have died of COVID-19 in the 47 states that reported data have been in nursing homes and assisted living centers, according to Kaiser Health News.
Kaiser Family Foundation
The question is whether nursing homes could have done better – and can do better going forward.
To some experts, there was probably little care facilities could have done. “This pandemic hit all nursing homes. It’s a lot more about where they’re located and how much traffic they had and the neighborhoods that got hit,” says Tamara Konetzka, a professor of public health at the University of Chicago.
Gaps and inconsistencies in reporting standards across states have also made it hard to reach clear conclusions. “There’s a lot of uncertainty around the data,” says Michael Barnett, an assistant professor at Harvard T.H. Chan School of Public Health in Boston.
Yet two state-level studies in Connecticut and California separately found that facilities employing more registered nurses did better at keeping their residents safe. The findings are consistent with other cross-state studies, which have also found that inadequate nursing staffing, including RNs, was a factor in COVID-19 outbreaks.
The staffing factor in COVID-19 outbreaks is persuasive, says Dr. Barnett. “I think the bottom line is that it seems like nursing homes that have worse staffing have more extensive outbreaks.”
It’s not the only relevant factor. In hotspots, even highly regarded homes weren’t spared. But it offers a potentially valuable confirmation of the idea that investing in senior nursing expertise, along with personal protective equipment (PPE) and testing capacity, could save lives.
Importance of registered nurses
Overall nurse staffing at RegalCare at Southport, a for-profit facility, is in line with the industry average in Connecticut. But it employs relatively few registered nurses. Payroll data for the first three months of 2020 show that its RNs averaged 20 minutes a day per resident, compared with the state average of 42 minutes.
That RN ratio seemed to be a factor in the disease’s spread in nursing homes in Connecticut, says Yue Li, a professor of public health sciences at the University of Rochester. He led a study of state data published in the Journal of the American Geriatrics Society. “A higher ratio is really helpful to identify and prevent disease,” he says.

Professor Li’s study modeled the impact of having fewer RNs. At homes in Connecticut with confirmed cases, a 20-minute increase in RN staffing was associated with 22% fewer cases. In homes with at least one death, a 20-minute increase was associated with 26% fewer deaths.
RNs are vital because they are the “top dogs” in facilities who oversee direct carers like Ms. Haschak and Ms. Polissaint and manage routine and emergency medical care. Particularly crucial during this pandemic, they are also typically in charge of infection control and for assessing residents.
“The reason why [registered] nurses are important is that they set a standard,” says Nicole Howell, executive director of Ombudsman Services of Contra Costa, Solano and Alameda in Northern California, which represents the interests of care home residents. “It’s about leadership.”
Inside one nursing home
RegalCare at Southport has been on a federal watch list since 2018 for a string of deficiencies, including citations for infection control. Homes on the list that fail to improve care standards can be barred from federal funding. As of July, RegalCare Southport still hadn’t improved, one of 27 such homes nationwide in that category. (The U.S. has around 15,400 federally regulated nursing homes.)
Ms. Polissaint has worked at the facility for 11 years. Even before the pandemic, she was frustrated at a lack of support for front-line carers from management. “We don’t have any support. Communication is very poor,” she says.
When Ms. Haschak was off sick for a month with COVID-19, she says her supervisors never called to check on her. Only Ms. Polissaint called and texted her.
By May, Ms. Polissaint was back on her wing, the designated COVID-19 section of the facility. She says the emotional strain of losing residents to the disease was compounded by their near-isolation at the end, as visitors weren’t allowed inside nursing homes.
“The worst part is the families weren’t able to come in and see them,” she says. They never saw how Ms. Polissaint and her aides cared for them, despite the shortages of masks and gowns and other equipment in the facility. “It was a hustle to get a mask,” she says.

In May this year, RegalCare at Southport was cited by state inspectors twice for COVID-19-related violations: On one visit, they found single-use protective suits being reused. On another, staff told inspectors that they couldn’t obtain masks, face shields, and other PPE, and a worker said she was given a brown paper bag to use as protection.
In response, Christopher Massaro, the facility’s executive administrator, said in a statement: “Regalcare at Southport has followed and continues to follow all CDC and State of Connecticut Department of Health guidelines for Covid 19 including the myriad of changes and updates they have made throughout this pandemic.”
On June 8, Gov. Ned Lamont ordered an independent inquiry into what had happened in nursing homes and assisted care facilities and whether more could have been done to protect residents from the coronavirus.
By late July, RegalCare had lost 19 residents, out of more than 2,500 deaths in Connecticut nursing homes. That put it in the middle of the pack on a per-bed basis.
A different experience
River Glen Health Center in Southbury, Connecticut, is a 45-minute drive from Southport. It has the same number of beds – 120 – and is part of a for-profit regional chain, CareOne. But it has significantly more RNs per resident, averaging 48 minutes in the first quarter.
When COVID-19 hit Connecticut in March, River Glen supervisors zeroed in on the risk of transmission both from staff and patients discharged from hospitals, says administrator Mary Noonan. They insisted that residents wear masks while receiving care. Nurses who worked in other health facilities were assessed for risk; others who had been on vacation were also monitored.
“We were trying not to have any contamination,” she says.
What helped, she says, was low staff turnover and having supervisors who knew them well and could be proactive at a time when testing and PPE were in short supply. The RNs “were invaluable. They knew how to be vigilant. They knew the procedures,” says Ms. Noonan.
So far, only three residents and two employees at River Glen have tested positive for COVID-19. None have died.
Not just a “bad apples” problem
To members of the industry, singling out nurse staffing misses the larger picture. They argue that operators followed federal guidelines and were blindsided by asymptomatic spread of an unknown virus and then left to fend for themselves as hospitals, not long-term care homes, got priority for PPE and testing.
For example, the Centers for Disease Control and Prevention initially required only nursing home staff who served residents who had tested positive for COVID-19 to wear masks. It changed its guidance on April 2 to include all staff.
“Even the highest quality organizations could not handle this [pandemic] because of where they were located and who the populations were in their building,” says Robyn Stone, senior vice president at LeadingAge, which represents nonprofit homes. “We have fabulous providers in New York that were filled with COVID.”
Some research supports this view. One study looked at more than 9,000 facilities and found that most outbreaks happened inside homes where the virus was prevalent in the outside community. The study, published in the Journal of the American Geriatrics Society, found no association with quality ratings or past infection problems.
“This suggests that COVID-19 is not a ‘bad apples’ problem, but a system-wide problem that can impact any nursing home in any state,” the study’s leader, David Grabowski of Harvard Medical School, told a U.S. House Ways and Means subcommittee hearing on June 25.
The effects of nursing levels
Yet many carers and experts say that nursing levels – and particularly RN levels – can have an important effect. While some key variables, like location, were out of nursing homes’ control, having a “strong RN, trained in up-to-date protocols” meant a facility was better prepared to respond, says Ms. Howell, the ombudsman in Northern California. “It matters what you do from there.”
Federal law requires one registered nurse to be present at nursing facilities eight consecutive hours per day, but there are no federal minimum levels for the ratio of RNs per resident. At least one licensed nurse – Ms. Haschak’s position – must be present at all times.
In 2018, Office of Inspector General for Health and Human Services found that nearly 1,000 nursing homes, or 7% of those surveyed, had failed to meet federal minimum staffing requirements for more than 30 days, mostly on weekends. “This raises concerns that some nursing homes may not have fully met their residents’ needs,” it wrote.

Decades of research shows that higher nursing staffing improves quality of care and that higher RN staffing in particular is associated with decreased infections and other positive indicators. Most states mandate a minimum overall staffing ratio. California sets a minimum of 3.5 hours of nursing care per resident, a standard that 1 in 4 homes failed to meet in 2017.
A recent study of California facilities found that those where RNs averaged less than 45 minutes a day per resident were twice as likely to have resident COVID-19 infections. Homes that had no infections had both higher RN and total staffing ratios compared with those that did, according to the study.
Charlene Harrington, who led the study, has spent decades studying how nursing homes are run and staffed, both in the U.S. and other wealthy countries. Now a professor emeritus at the University of California, San Francisco, she says that quality of care and inadequate staffing contributed to the severity of the outbreak in California’s nursing homes. Her study found that some nursing home operators substitute for RNs with nurses with less training as a way to keep down costs.
More than a pizza party
After recovering, Ms. Haschak went back to work in May. The nursing home had fewer residents, but her wing was still short-staffed and there wasn’t enough PPE.
Her facility wasn’t alone: Around 1 in 5 nursing homes nationally reported being short of staff and lacking protective gear like N95 masks in May, according to federal data.
In June, she was asked by her union to speak at a House Ways and Means hearing on the nursing home crisis. Ms. Haschak spent days practicing her speech, trying not to break down as she recounted her experience. Her teenage daughter encouraged her to keep going. “You can do it,” she told her.
On June 25, she sat on her sofa and spoke via video link to the committee.
“Thank you for allowing me to share my story today,” she began, her voice wavering. “My name is Melinda Haschak. I’m a nursing home worker from Stamford, Connecticut. I’ve worked in the health care industry for over 20 years.”
She went on to describe the conditions at her facility and what she felt was the lack of support from managers, and how she had to scrounge money to buy thousands of surgical masks for the staff, before she got sick with COVID-19. Then she calmly spoke of the continued strain caused by understaffing and shortages of PPE, and not knowing which residents had tested positive.
Nurses have received food donations, she added. Staff also received extra hazard pay in May and June. But that’s no substitute for decent wages and conditions, she told the committee.
“My co-workers and I do not need a pizza party,” she said. “We need PPE.”
Staff writers Sarah Matusek and Kelsey Olya Evans contributed to this report.
Editor’s note: As a public service, we have removed our paywall for all pandemic-related stories.




